
From 1 December 2022, ramipril (brand name: Tryzan) became fully funded without restriction and can be prescribed for any relevant use. These uses include hypertension, heart failure, progressive kidney disease, diabetic kidney disease, and prevention of cardiovascular events in those with established heart disease.
Mr Fapuleai is a 65-year-old Samoan man who has an appointment to renew the script for his regular medications. He has diagnoses of hypertension, hyperlipidaemia, and prediabetes.
Current medications:
Cilazapril 5mg orally once daily
Felodipine 5mg orally once daily
Atorvastatin 40mg orally once daily
He is stable on these medications with a blood pressure today of 130/74mmHg. Home readings sit below 130/80mmHg. Recent bloods show normal renal function. You calculate his creatinine clearance (CrCL) to be 55mL/min.
You explain to Mr Fapuleai that cilazapril is going off the market in mid 2023, and discuss the need to change to a different ACE inhibitor.
Ramipril mechanism of action
Ramipril is a prodrug and is hydrolysed into the active metabolite ramiprilat, which has a long half-life allowing once-daily dosing.
ACE inhibitors reduce the conversion of angiotensin I to angiotensin II and inhibit the breakdown of bradykinin. This reduces vascular smooth muscle vasoconstriction, increases renal excretion of sodium and water thus reducing blood volume and blood pressure, and is nephroprotective via reducing filtration pressure in the kidneys.2
Safety and side effects
Ramipril shares common side effects, cautions, contraindications, and interactions with all other ACE inhibitors.1,3
Common side effects include:
Dry, persistent cough
This is the most common side effect of any ACE, experienced by around 11% of patients. This is more common in women, and often worse lying down and/or at night. Cough is generally a class effect of all ACE inhibitors. If cough is troublesome on one ACE inhibitor, changing to a different anti-hypertensive class may be required.
Alternatively, a change in anti-hypertensive class may be required.
Hypotension
This can occur with the first dose and with escalating doses, and particular caution is needed in those also on diuretic medications or who are volume deplete.
To avoid this initial drop in those on diuretics, the diuretic may be withheld for 2-3 days prior to starting then re-introduced. If this isn’t possible, consider a lower initial dose of 1.25mg.
Renal impairment
It is likely that serum creatinine will slightly rise after starting an ACE inhibitor. If creatinine rises more than 30% from previous baseline, or eGFR drops by more than 25%, the dose should be reduced or stopped and other causes for decline investigated.
If serum potassium rises to greater than 5.9mmol/L the drug should be stopped.
For an extensive list of side effects see the New Zealand Formulary (NZF) monograph on ramipril, ‘adverse effects’ section.
Cautions
Age - must be over 18 years
Ramipril is not approved for use in those younger than 18 years old. The only ACE inhibitors in New Zealand currently licensed for use in children are lisinopril, captopril, and enalapril.4
Pre-existing hepatic impairment
Hepatic metabolism of prodrug ramipril to ramiprilat is delayed when liver function is impaired. This leads to increased plasma ramipril levels, and therefore the maximum dose should be 2.5mg per day. Close monitoring is required in those with established liver impairment.
This is also relevant for prodrugs enalapril, perindopril, and quinapril. Lisinopril and captopril are not prodrugs, so may be a better choice if liver issues are a concern.1,2,5
Pre-existing renal impairment
Initial and maximum doses are guided by CrCL:
- CrCL >50mL/min - no dose adjustments needed
- CrCL 20-50mL/min - start at 1.25mg, maximum daily dose 5mg
- CrCL <20mL/min - avoid.1,2,5
MDCalc has a user-friendly CrCL calculator which provides an adjusted value for BMI if height is available
Never overlook the “Triple Whammy”
The combination of an ACE inhibitor, diuretic, and non-steroidal anti-inflammatory drug can be dangerous due to risk of acute kidney injury. If at all possible this combination should be avoided. If unavoidable, close monitoring or renal function is recommended.1.6
Pregnancy
Exclude pregnancy before starting treatment.
ACE inhibitors should be avoided at all stages in pregnancy, however, the evidence of fetal harm is strongest for the second and third trimesters where they can cause severe toxicity including fetal renal failure and death.
If a woman becomes pregnant while on an ACE inhibitor, this should be stopped and changed to an alternative immediately.1,5
Breast-feeding
The manufacturer advises to avoid. Although NZF suggests ACE inhibitors can be considered after the first few weeks of life in a healthy-term infant, there is no current data available on ramipril in breastfeeding.
Newborns can be more susceptible to the effects of ACE inhibitors such as hypotension and oliguria. Until more data is available, it may be preferred to avoid ramipril in breastfeeding and use an alternative drug, especially in newborns and pre-term infants.
Contraindications
- Hypersensitivity to a previous ACE inhibitor
- Previous angioedema - idiopathic or hereditary
- Hypotension
- Concurrent use with an angiotensin receptor blocker (ARB) or Entresto
- Pregnancy
- Severe bilateral renal artery stenosis 2
Pertinent interactions for a primary care setting
|
Interacting drug/class |
Potential risks |
| ARB | Renal impairment, hypotension, hyperkalaemia |
| Entresto | Angioedema, renal impairment |
| Allopurinol | In the context of pre-existing renal impairment: leucopaenia, hypersensitivity |
| Lithium | Increased Lithium levels |
| Spironolactone | Hyperkalaemia |
The benefits and risks of different ACE inhibitors are very similar across the class.3
A practical approach for starting or changing to ramipril
Tryzan comes in capsule form with available strengths of 1.25mg, 2.5mg, 5mg, and 10mg. The capsules cannot be split or halved. It can be taken with or without food.1
Starting de novo
- Identify a clear clinical indication.
- Obtain the baseline blood pressure and renal function.
- Check for interactions or contra-indications.
- Prescribe ramipril at the recommended starting dose as per the NZF - the initial dose depends on the indication and CrCL.2
- Arrange renal function 1-2 weeks after starting, followed by a clinic appointment to check blood pressure and toleranc.
- Titrate dose as required.
Changing from another ACE inhibitor or ARB
- Identify and discuss the rationale for changing (e.g. currently on cilazapril).
- Discontinue current ACE inhibitor or ARB.
- Identify the equivalent dose of ramipril.
- Start ramipril to take at the same time the next dose would be due.
- Arrange renal function 1-2 weeks after starting, followed by a clinic appointment to check blood pressure and tolerance.
- Titrate dose as required.
Equivalent dosing for ACE/ARB medicines
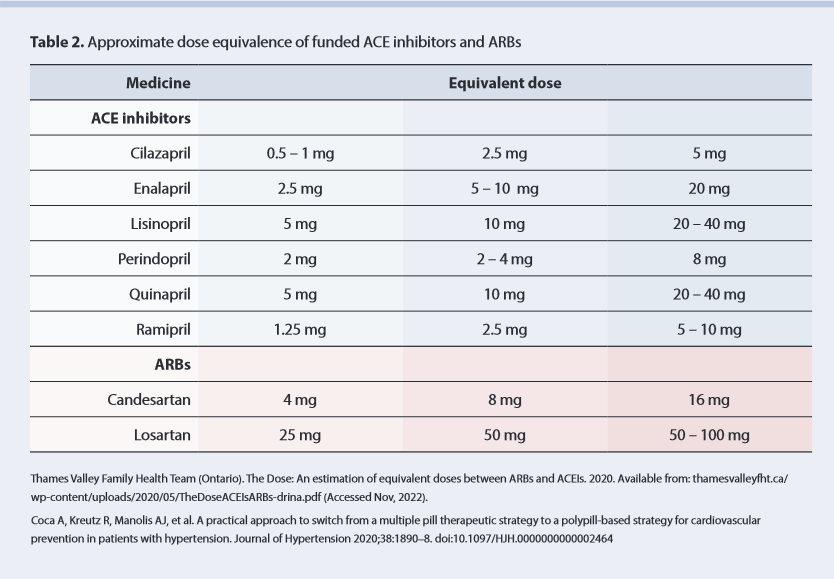
From Reference 3: Prescribing ACE inhibitors: time to reconsider old habits bpacnz (2022)
You describe Tryzan to Mr Fapuleai as a ‘cousin’ of cilazapril that he can safely change to at an equivalent dose. This will work in a similar way to maintain control of his blood pressure.
After discussing dosing and safety information, you relay the plan below:
- Stop cilazapril.
- Start ramipril at an equivalent dose of 10mg (1 tablet) once daily the following day.
- Get a blood test 1-2 weeks after starting ramipril to check kidney function.
You arrange for Mr Fapuleai to come back in two weeks after the blood tests to recheck blood pressure, and discuss any issues that arise with the transition.
Practice points
- Cilazapril is no longer available from mid 2023 and all patients must be changed to an alternative medicine.
- Ramipril (Tyrzan) is a newly funded ACE inhibitor that has equivalent indications, side effects, contra-indications and cautions to all other ACE inhibitors.
- Ramipril can be started de novo or, if changing, at an equivalent dose to another ACE inhibitor or ARB.
- Monitoring requirements include baseline renal function to guide initial dosing, and follow-up renal function 1-2 weeks after starting or changing dose.
This MedCase was written by Dr Hazel Wilks (MBChB), with expert review by Dr Hari Talreja, Consultant Renal Physician, MD, DNB, MPH (Harvard), FRACP.
Recognition of Learning Activities
Don't forget to log your time with The Royal New Zealand College of General Practitioners portal for recognition of learning activities.

