
Metabolic syndrome is a cluster of interrelated metabolic risk factors that significantly increase the risk for cardiovascular disease and type 2 diabetes mellitus. The prevalence of metabolic syndrome in New Zealand is notably high, particularly among Māori and Pacific Island populations1,2. This disparity reflects complex interactions between genetic predisposition, social determinants of health, and systemic barriers to healthcare access.
This MedCase explores the identification, treatment/prevention, and complications of metabolic syndrome.
This case illustrates the natural history of untreated metabolic syndrome progressing to type 2 diabetes (T2D) and heart failure with preserved ejection fraction - complications that are disproportionately common in Pacific Island populations. Early identification and sustained treatment of metabolic syndrome can prevent these outcomes.
Sione is a 45-year-old Tongan man who presents to your practice as a new patient. He recently moved to the area and works full-time as a truck driver. He has not seen a doctor in years and was advised by his boss to get a check-up after a colleague had a heart attack at work.
- Past medical history: None documented
- Medications: None
- Social history: Non-smoker, occasional alcohol use, sedentary occupation with limited physical activity.
- Family history: Father died of myocardial infarction at age 58; mother had T2D, diagnosed in her 40’s.
Physical examination:
- Height: 178 cm; Weight: 112 kg; BMI: 35.4 kg/m²
- Waist circumference: 108 cm
- Blood pressure: 142/88 mmHg (confirmed on repeat)
- Cardiovascular and respiratory examination: unremarkable.
Sione was sent for full blood work and was booked for follow-up in 2 weeks' time, with a CVD risk assessment with the practice nurse beforehand.
Understanding metabolic syndrome
The harmonised diagnostic criteria require the presence of any three of the following five components3:
- Elevated ethnic‑specific waist circumference
- Elevated triglycerides: ≥1.7 mmol/L or on medication
- Reduced HDL cholesterol: ≤1.0 mmol/L in men, ≤1.3 mmol/L in women
- Elevated blood pressure: ≥130/85 mmHg or on antihypertensive medication
- Elevated fasting glucose: ≥5.6 mmol/L or on glucose-lowering medication
Patients with metabolic syndrome are at twice the risk of developing cardiovascular disease over 5-10 years and have a 5-fold increased risk of developing T2D compared to those without the syndrome4. Early treatment of metabolic syndrome reduces the risk of developing T2D and/or cardiovascular disease.
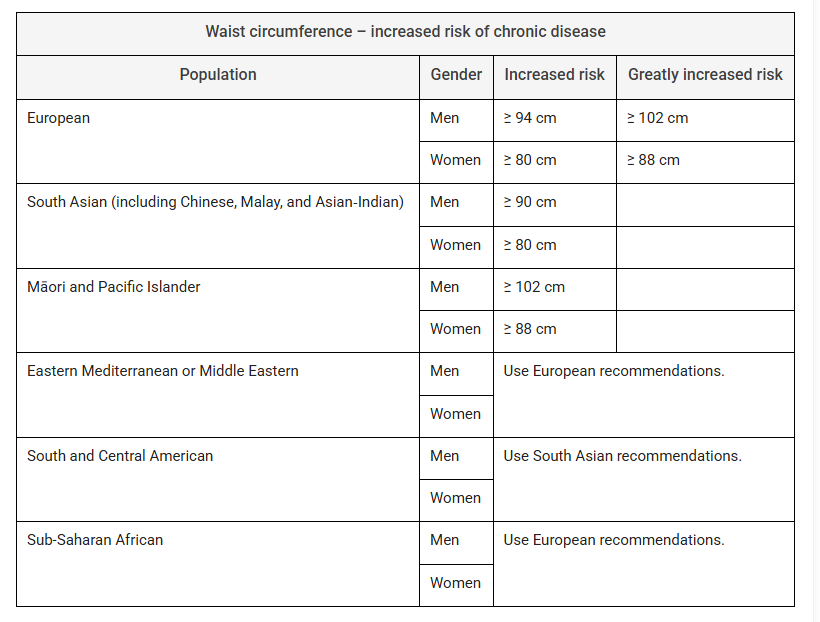
(Table collated from The IDF consensus worldwide definition of the Metabolic Syndrome, p11 and Clinical Guidelines for Weight Management in New Zealand Adults p4)
Sione's initial laboratory results:
- Fasting glucose: 6.2 mmol/L
- HbA1c: 55 mmol/mol (7.2%) - meets criteria for T2D
- Total cholesterol: 5.8 mmol/L; LDL cholesterol: 3.8 mmol/L; HDL cholesterol: 0.9 mmol/L; Triglycerides: 2.4 mmol/L
- eGFR: >90 mL/min/1.73m²
- Urine albumin: creatinine ratio: 0.8 mg/mmol.
Sione meets all five criteria for metabolic syndrome:
✓ Elevated waist circumference: 108 cm (threshold ≥102 cm)
✓ Elevated triglycerides: 2.4 mmol/L (threshold ≥1.7 mmol/L)
✓ Reduced HDL cholesterol: 0.9 mmol/L (threshold ≤1.0 mmol/L)
✓ Elevated blood pressure: 142/88 mmHg (threshold ≥130/85 mmHg)
✓ Elevated fasting glucose: 6.2 mmol/L (threshold ≥5.6 mmol/L) with HbA1c 55 mmol/mol - meets criteria for T2D.
His PREDICT CVD risk is calculated by the practice nurse to be >15%.
Management
Lifestyle modification: First-line therapy

Lifestyle modification is the cornerstone of metabolic syndrome management5. The goals include:
- Weight loss: Target 5-10% reduction in body weight over 6-12 months.
- Dietary changes: Mediterranean-style diet emphasising fruits, vegetables, whole grains, legumes, fish, olive oil, and limited red meat.
- Physical activity: Minimum 150 minutes of moderate-intensity activity per week (e.g. Green Prescription).
- Behavioural support: Structured programmes with trained health professionals (e.g. Health Coach).
Pharmacotherapy
There is no specific pharmacotherapy for metabolic syndrome itself; however, medications are indicated to address individual risk factors including lipids, blood pressure, and diabetes.
Lipid management
For patients with 5-year CVD risk ≥ 15%, the 2018 NZ Consensus Statement recommends LDL ≤1.8 mmol/L. An updated target of <1.4 mmol/L is increasingly used in clinical practice, including in the NZSSD guidelines for diabetes. In primary prevention, use a statin (e.g. Atorvastatin in doses up to 40mg as tolerated).
Statin intolerance, especially myalgia, is overdiagnosed. There is good evidence from placebo-controlled trials that most perceived statin intolerance is not an adverse effect of statins. Many, but not all, patients with possible adverse effects can be rechallenged successfully6.
Blood pressure management
In young patients and those with a high CVD risk or coexisting comorbidities (e.g., diabetes mellitus, chronic kidney disease, coronary artery disease, left ventricular hypertrophy), the ideal target is ≤130/80 mmHg.
Angiotensin receptor blockers (ARB) should be initiated (e.g. Candesartan 8 mg daily) and titrated as tolerated to reach target. Check electrolytes and creatinine 2 weeks after initiating or increasing the dose of an ARB.
Diabetes management
Metformin 500 mg twice daily should be initiated and titrated as tolerated.
Given Sione's cardiovascular risk profile and findings from the last consultation, you discuss and initiate treatment, including Atorvastatin for lipids, Metformin for diabetes, and Candesartan for blood pressure and renal protection.
This was alongside lifestyle interventions. The local recreational centre facilitates both health coaching and green prescription. Sione was interested in this, as a few of his church congregation also attended.
You arrange for Sione to return in three months.
At Sione's 3-month check, he is showing modest but meaningful improvements:
- Weight: 108 kg (4 kg loss)
- Waist circumference: 105 cm (3cm reduction)
- Blood pressure: 132/82 mmHg
- HbA1c: 42 mmol/mol (6.0%) - improved glycaemic control
- LDL cholesterol: 3.2 mmol/L
- Triglycerides: 2.0 mmol/L
He reports attending Green Prescription sessions regularly and making dietary changes with his health coach's support.
His medications are well-tolerated.
Management of cardiovascular complications of metabolic syndrome
Patients with metabolic syndrome are at twice the risk of developing cardiovascular disease over 5-10 years.
This includes coronary heart disease, myocardial infarction, stroke, heart failure, peripheral artery disease, and cardiac arrhythmias.
You have not seen Sione for 12 months when he presents acutely to your clinic. Sione admits he stopped taking his medications 6 months ago due to cost, and stopped attending health coaching due to increased work hours. He has been having financial obligations from supporting his parents in Tonga.
Symptoms
- Progressive shortness of breath over 2 weeks, now limiting speech to short sentences.
- Marked orthopnoea (requires 3 pillows or now unable to lie flat).
- Paroxysmal nocturnal dyspnoea with frequent nocturnal breathlessness.
- Bilateral leg swelling extending to knees.
- Reduced exercise tolerance - now breathless on minimal exertion or at rest.
- Occasional dry cough and feeling of chest “tightness”.
Physical examination
- Weight: 115 kg
- Blood pressure: 156/92 mmHg
- Pulse: 104 bpm, regular
- Respiratory rate: 26 breaths/min, SpO₂ 91% on room air
- Cool peripheries and mild diaphoresis
- Bibasal crackles rising to mid-zones on chest auscultation
- Elevated jugular venous pressure to angle of jaw at 45°
- Enlarged tender liver
- Bilateral pitting oedema to mid-calves.
Due to the severity of symptoms, he is admitted acutely to hospital for suspected congestive heart failure with fluid overload.
He was in the hospital for 5 days. The discharge summary is sent to your inbox with the following diagnosis, investigations, and medications.
Diagnosis: Acute decompensated heart failure (likely HFpEF) with worsening T2D and early diabetic kidney disease.
Blood tests:
- HbA1c: 70 mmol/mol- (worsened glycaemic control)
- NT-proBNP: 850 pg/mL (elevated, consistent with heart failure)
- eGFR: 78 mL/min/1.73m² (decline from >90).
Echocardiogram results:
- Left ventricular ejection fraction: 55% (preserved)
- Grade 2 diastolic dysfunction
- Consistent with heart failure with preserved ejection fraction (HFpEF).
Discharge medications:
- Atorvastatin 40mg OD
- Metformin 1000mg BD
- Candesartan 16mg OD
- Furosemide 20mg OD
- Empagliflozin 10mg OD.
You note empagliflozin special authority for funding under the T2D criteria.
Evidence-based therapy: Empagliflozin
Empagliflozin (Jardiance) is available under special authority for Heart Failure with reduced Ejection Fraction and for T2D. However, it also has benefits in patients with HFpEF.
For patients with HFpEF who do not have T2D, empagliflozin is not currently Pharmac-funded, so patients may need to self-fund.
The EMPEROR-Preserved trial demonstrated that empagliflozin 10 mg daily in patients with heart failure and ejection fraction >40% resulted in:
- 21% reduction in the composite endpoint of cardiovascular death or hospitalisation for heart failure (HR 0.79, 95% CI 0.69-0.90, p<0.001)
- 29% reduction in hospitalisation for heart failure (HR 0.73, 95% CI 0.61-0.88, p<0.001)
- 27% reduction in total heart failure hospitalisations
- Benefits were consistent regardless of diabetes status7.
SGLT2 inhibitors reduce heart failure hospitalisations and may improve quality of life in patients with symptomatic HFpEF, independent of glucose-lowering effects, making them a core therapy alongside diuretics and risk factor control.
Additional benefits in T2D and Chronic Kidney Disease
Beyond heart failure benefits, empagliflozin provides:
- Improved glycaemic control with modest HbA1c reduction.
- Renal protection across a wide range of eGFR values, including reduction in kidney disease progression (HR 0.72, 95% CI 0.64-0.82).
- Cardiovascular risk reduction, including reduction in cardiovascular death.
- Modest weight loss (typically 1-2 kg).
- Low risk of hypoglycaemia when used without insulin or sulfonylurea8.
Monitoring parameters:
- Volume status and blood pressure (risk of hypotension with diuretic effect).
- Renal function (may see initial small decline in eGFR, which stabilises).
- Genital and urinary tract infections (increased risk, particularly in women).
- Diabetic ketoacidosis (rare but important to counsel about sick day management).
Sione returns to your clinic a few weeks after discharge. He has been adherent to medications and reports feeling "much better."
- Weight: 111 kg (4 kg fluid loss)
- Blood pressure: 136/84 mmHg
- No peripheral oedema
- Improved exercise tolerance
- Sleeping flat without orthopnoea.
You arrange ongoing follow-up with cardiology and diabetes services and reconnect him with his health coach for continued lifestyle support.
Practice Points
- Metabolic syndrome is highly prevalent in Māori and Pacific Island populations in New Zealand, requiring culturally appropriate screening and intervention strategies.
- The harmonised diagnostic criteria require any three of five components: elevated waist circumference, elevated triglycerides, reduced HDL cholesterol, elevated blood pressure, and elevated fasting glucose.
- Lifestyle modification is the foundation of metabolic syndrome management, with emphasis on weight loss, Mediterranean-style diet, and regular physical activity.
- Statin therapy is recommended for patients with metabolic syndrome and elevated cardiovascular risk. New Zealand uses absolute cardiovascular risk assessment (PREDICT calculator) to guide treatment decisions. For 5-year CVD risk ≥15%, statin therapy is recommended. For risk 5–15%, benefits and risks should be considered on an individual basis.
- SGLT2 inhibitors provide dual benefits in patients with both T2D and HFpEF, reducing heart failure hospitalisations, cardiovascular death, and kidney disease progression independent of glucose-lowering effects.
- Early recognition and sustained treatment of metabolic syndrome can prevent or delay progression to T2D and cardiovascular complications.
- Social determinants of health, including medication costs and competing family responsibilities, significantly impact treatment adherence and outcomes in Pacific communities. Addressing these barriers is essential for effective chronic disease management.
This MedCase was written by Dr Anthony Dewan MBChB, FRNZCGP, with expert review by Dr Gerry Wilkins, Consultant Cardiologist.
References
Supported with an unrestricted educational grant from
Recognition of Learning Activities
Don't forget to log your time with The Royal New Zealand College of General Practitioners portal for recognition of learning activities.

